 Introduction:
Introduction:
Melanocytes are the cells responsible for pigmentation and coloring of skin among individuals, the component being known as ‘melanin’. These cells are present in the basal layer of the epidermis (the outermost layer of the skin). Melanoma is the most dangerous form (although less common, around 2% of the total number of cases of skin cancer, are due to melanoma) of cancer that originates from the melanocytes. It is responsible for around 75% of deaths in people affected with melanoma. Other types of skin cancers which lead to malignancy include basal and squamous cell carcinoma.
The roots of melanoma lie in the irreversible damage caused to the DNA of the cells lining the skin, mostly due to exposure to UV radiation with respect to the skin coloring of people. Hence, a geographic distribution is seen as far as the rates of incidence of melanoma are concerned .Melanoma has been seen to affect white people, as much as 20 times more than African Americans. Studies suggest that, mostly Caucasians from Northern and North Western Europe, where the climate is on the sunnier side, are affected with melanoma. However, high incidences are also found in Northern and Latin America, Europe, Oceania and Southern Africa.
The rates of melanoma have been increasing steadily for the past 30 years. Melanoma most commonly originates from the moles on one’s body, but that does not imply upon the fact that people with moles always end up with melanoma, as moles are mostly benign outgrowths on the epidermis (Some moles like the Spitz Nevus resemble melanomas in appearance, especially in children and teenagers, but are actually not melanomas. An expert opinion is always warranted before taking any action on them. However one may be advised to get it removed, just to be on the safer side. Other examples of benign tumors arising from moles include Seborrheic keratoses, with a waxy texture, Hemangiomas, which are benign blood vessel outgrowths often reddish or pinkish in color, lipomas and warts caused as a result of viral infections mostly).
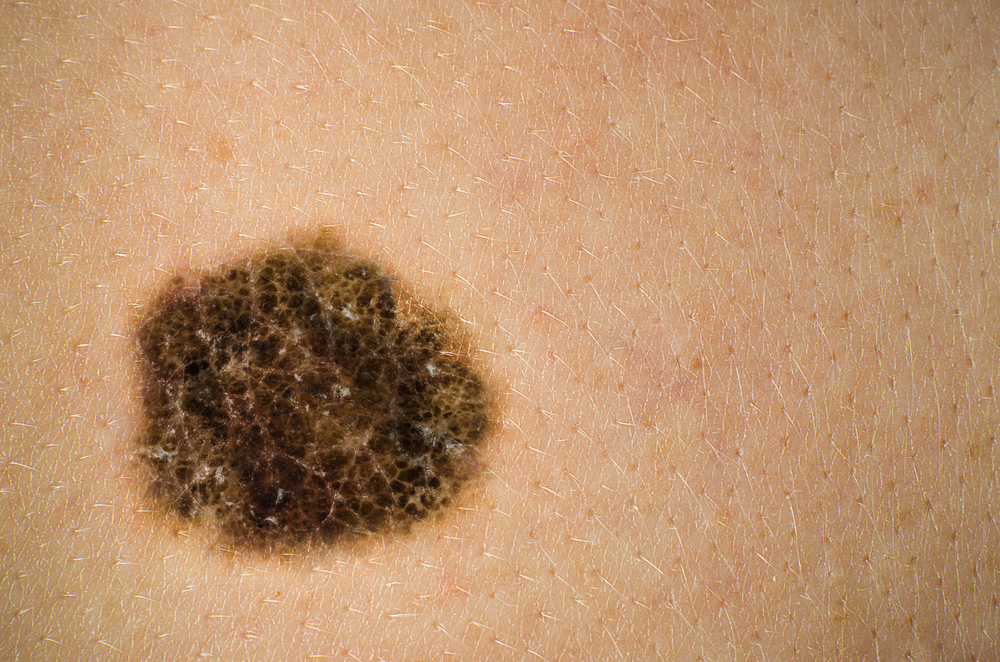
Melanomas are generally black or brown in color but some of them may be white, red or pink in appearance depending on their origin and location on the body. The most common site for development of melanomas in men is the trunk (including the chest and the back) followed by surfaces on the head and neck, space between shoulders and hips, whereas those in the lower legs are warning signs in women, along with the shoulders and hips. Although white people are affected in high numbers as compared to people with a darker complexion, the risk of developing melanoma in the palms of the hands, soles of feet and under the nails is equal among populations with a darker skin tone as well. In fact, it has been seen that African Americans pick up the disease in these areas a lot more than white people. The neck and face also are common sites for development of these malignant lesions. Previous studies have shown that melanoma has been responsible for 9710 deaths in the United States of America, annually.
Predominantly, melanoma affects the skin, but in rare cases melanoma also affects other organs where it is present (like the bowel and the eyes).There are three common types of melanoma, namely, cutaneous melanoma, mucosal melanoma and ocular melanoma. If treated at its early stages when the cancer has not spread to the inner layers and is thin, it is almost entirely curable provided the affected area is completely removed. But if it proceeds towards advanced stages, special therapeutic care is needed, mostly in the form of radiation therapy, chemotherapy or immunotherapy in combination with or without each other, coupled with surgery.
 Epidemiology:
Epidemiology:

Melanoma is a growing cause of concern and a public health burden in the United States, with the number of cases rising every year. According to statistics from the American Cancer Society, in 2014 the estimated number of cases diagnosed would be around 76,100, with about 43,890 cases expected in men and 32,210 cases expected in women, and the number of deaths caused as a result of malignant, metastatic melanoma would range up to 9710 people, with 6470 men and 3240 women. Melanoma has been stated as the fifth most common form of cancer amongst men (accounting for 5% of the new cases diagnosed annually) and the sixth among women (accounting for 4%of all new cases of malignancy annually). According to data accumulated form studies conducted by the National Institutes of Health from 2009 till 2011, around 2.1% of men and women living in the United States are expected to be diagnosed with melanoma at some point of life. However, the average five year survival rates for people living in the US is 91.3%, a lot better than the other Caucasian populated territories.
Though most common among people living in Australia and New Zealand (it being the third highest cause of cancer in Australia), the rates of incidence among people in the United States have been on a steady rise ever since the 1930s. Back then, the life time risk of developing malignancy due to skin cancer was 1 among every 1500, which, due to a steady increase by 5% to 7% every year, was 1 among 75 in the year 2000, and has now reached 1 in every 59 people. Melanoma, causing deaths thrice as much as other skin cancers, has had an increase in the mortality rates by 2% annually, as well, ever since 1960. It continues to rise every year, with the rates being faster than any other kind of cancer, other than lung cancer in women. Queensland (Australia) shows the highest rates of incidences with 57 cases per 100,000 and very high death rates, mounting to as many as 7.3 to 9.8 per 100,000 people, closely followed by Israel, with incidence rates of 40 cases per 100,000 annually. On a global basis, studies from 2012, Melanoma has been responsible for as many as 55,000 deaths among 232,000 new cases.
Melanoma is more common among white people with fair skin tones. Dark skinned Caucasians have a lower risk of developing melanoma as compared to their fairer counterparts. Getting sunburnt as compared to tanning, can be a sure indicator for melanoma among people with a lighter complexion. Also, people with beach blonde and red hair with a lot of freckles, tend to be more prone to developing melanoma. White people have the highest incidence in Hawaii, with 20 to 30 cases per 100,000 annually.
Melanoma is slightly more common in males than in females, and it is more common among professional than unskilled workers. Women tend to get diagnosed mostly between ages 25 and 29, and have lesions which are non-nucleated and are thinner than those present in men. It causes as many as 7000 deaths annually among women itself. Unlike other forms of cancer, melanoma is known to affect the younger population more frequently than the older ones, with 75% of the patients being middle aged or younger adults, less than 55 years of age. The median age of diagnosis is 57 years. Children aged as less as 10 years can also develop a de novo form of melanoma though this is very rare.
 Etiology:
Etiology:

Melanoma can arise from previously existing lesions or due to exposure to risk factors. The main cause of melanomas is exposure to harmful ultraviolet rays (UV lights), but other risk factors like smoking, genetic factors, excess sun exposure, frequent tanning sessions can also contribute to the development of skin cancer. Though, many people are exposed to these factors due to professional reasons or as a part of their daily lifestyle, it is not mandatory that they will develop skin cancer. It only implies that these people are more prone to developing skin cancer than people who are not exposed to these risk factors.
- Exposure to UV light: Different wavelengths of UV light affect the skin in different ways, inducing damage in the form of DNA breakage, induction of cell division of melanocytes, free radical production, suppression of the immune system and impairment of healing mechanism of the skin to name a few. The most common ways of getting exposed to UV rays include sunlamps, tanning beds and exposure to UV radiations as a result of irradiations at radiology clinics. People working in airplanes also have a greater risk of developing skin cancer due to increased exposure to UV light. A survey conducted by the International Agency for Cancer Research suggests that people who start using tanning beds and sunlamps before the age of 30 are at 75% more risk of developing skin cancer (melanoma). The most harmful wavelengths of UV lights include UVB rays, having frequencies between 280 and 315nm and UVA rays having higher wavelengths between 315 and 400nm. These rays induce dimer formation between two consecutive pyrimidine bases via a DNA strand (a phenomenon known as cyclobutane pyrimidine dimers (CPDs) formation – a type of direct DNA damage) that causes sunburn and production of melanin.
- Genetic Factors: Genetic mutations, either induced or passed on as a result of family history, also affect development of malignant skin cancers among people. There are genes which undergo mutations to induce irreversible damage to DNA that directly leads to the formation of melanoma, whereas others encode for factors which increase the risk of developing the same. A gene, CDKN2A (Cyclin Dependent Kinase Inhibitor 2A), responsible for regulation of the transcription factor p53 (a tumor suppressor protein which controls the damage and repair mechanisms of the cells, regulating the cell cycle and preventing the same from proceeding towards tumor formation), gets mutated in different ways, which paves the way for melanoma. A frame shift mutation occurs in the gene sequence due to insertion or deletion of nucleotides due to a host of factors (UV light exposure being one of them, as discovered recently), leading to altered production of the transcription factor (the pivotal p53 protein), triggering malignant melanoma. Another mutation of the same gene which results in the inhibition of the cell division due to modification of CDK4 (another cyclin dependent kinase involved in regulating the cell cycle). Recently, another gene, BRAF has been studied to play a major part in development of melanomas. It has been termed as a ‘switch’ gene known to trigger development of tumors once regulated abnormally. Some genes like MC1R which is responsible for red hair in people (which acts as a risk factor among many) can also be looked upon as predisposing factors for development of melanomas.
- Family History: Having two or more first degree relatives who have had melanoma, increases a person’s risk of developing melanoma in the later stages. Apart from this anybody who has had skin cancer previously, is more prone to develop malignant melanoma at some point. Family members or first degree relatives who have had inherited disorders like Xeroderma pigmentosum (XP) (an inherited disorder which impairs the person’s ability to produce an enzyme responsible for the repair of any kind of damage to DNA) that make the skin more prone to damage, are also at an increased risk of developing melanoma.
- Moles: Certain moles and mole-like lesions are considered to be predisposing factors of melanoma, especially in people with a family history of melanoma. One such mole (nevus) is the Dysplastic nevi, which might have a few features of melanomas, being larger in size and abnormal in color compared to its normal counterparts. It increases a person’s lifetime risk of developing melanoma by 10%, and the more of these moles on the skin, the more chances are that the person will be diagnosed with melanoma. On the other hand, not many of these nevi develop into malignant forms during a lifetime. So it is advisable to get an expert analysis done by a dermatologist before concluding upon anything. Another such mole is the Congenital melanocytic nevi, which is present in an individual at the time of birth. They increase the lifetime risk of melanoma by 0 to 10%, with a larger size denoting a higher chance of malignancy in the future. These can be surgically removed after consultation, before they can become cancerous in nature, but that depends on the size and location of the same. Some studies have also shown that having more than 50 common moles (with a round, overall smooth surface resembling that of a pea, but smaller in size, being pink, tan or brown in color) increases one’s chances of malignancy.
- Over exposure to Sun rays and tanning: Intense sunburns, blisters or having a lifetime exposure to sunlight and UV rays considerably increases one’s risk of getting skin cancer. Tanning booths and laser treatments are other sources of UV radiations which pose perpetual threats for development of melanomas.
- Co-morbidities and their medications (anti-depressants, antibiotics, hormones and steroids) which suppress the immune system, also make the skin more susceptible to melanoma.
- Smoking: Smoking induces several irreversible changes in the human DNA and is known to make people prone to a number of malignancies, skin cancer (melanoma) being no different.
 Types of Melanoma:
Types of Melanoma:

There are four basic types of melanomas, out of which three are non-invasive in nature and remain confined to superficial coverings of the skin. One is invasive and spreads to internal organs.
- Superficial spreading melanoma as suggested by the name is confined to the superficial layers of the skin, and is the most common (70%) of all forms of skin cancer. They are seen mostly in youngsters and remain confined to the outer layers of the skin for a long time before penetrating inwards. It starts with an irregular, rough, slightly elevated, (tan, brown, black, red, blue or white) colored patch that slowly spreads. The lesions are thin initially but become thicker with the gradual passage of time. It might begin from a benign mole (or a dysplastic nevus) or from normal skin.
- Lentigo maligna or Lentiginous melanoma is a common term used to indicate sun burnt skin, and is another form of non-invasive skin cancer. It usually remains limited to its place of origin for quite a long time. Lentigo maligna appears as a flat or slightly elevated, black, brown or tan colored patch, which consists of malignant cells which do not penetrate the deeper layers of the skin initially. This form of skin cancer is common among the elderly, with sun exposed skin or sunburns. The most common sites of appearance of these patches include the face, ears, upper trunk and forearms. Though it remains non-invasive for a long time, once left untreated, it leads to an invasive form of malignancy, known as Lentigo Maligna Melanoma. It begins like a papule from the darkened areas on the skin and proceeds towards the inner layers of the epidermis.
- Acral lentiginous melanoma is another form of skin cancer which is common among dark skinned and black ethnic groups, instead of the usual Caucasian race. It is more progressive as compared to lentigo maligna or superficial melanoma. The condition is marked by the appearance of brown to black, slightly elevated patches of discolored skin under the toe nails, on the palms of the hands or soles of the feet or sometimes on the oral mucosa. Non-hair bearing body parts and those not exposed to sunlight are mostly affected. This form of melanoma is the most common among African Americans and Asians with the mean age of detection being sixty to seventy years.
- Nodular melanoma is the most aggressive and invasive form of skin cancer, affecting 10 to 15% of the total number of cases. It tends to penetrate the skin more than grow in diameter. It is normally detected at very late stages because of this tendency to grow in depth instead of width. It commonly arises as a dark nodule (might be brownish or colorless as well, the latter case being one of the reasons it escapes first hand detection) from places with no initial signs of melanoma or any benign moles. Frequent places of development of such nodules include the trunk, legs and arms of the elderly. The lesion might be ulcerated and cause bleeding occasionally.
- Apart from these four, there are some other rare forms of melanoma including desmoplastic melanoma (a rare, deeply infiltrating variant of melanoma), soft tissue melanoma (affecting the soft tissues of the body) and amelanotic melanoma (a condition where the ability of the skin cells to make melanin is impaired).
 Diagnosis:
Diagnosis:

One should consider a patient’s family history before drawing any conclusion on the patient’s condition. It is advisable that people get themselves tested by a dermatologist at the earliest signs of possible melanoma (unusual skin darkening, moles, burns and so on). Patients belonging to families with a history of melanoma or even pancreatic cancer of astrocytoma (these two conditions also have similar genetic mutations as found in patients with melanoma) are at a higher risk and so are those who themselves have had a history of melanoma before. This is because there have been cases of patients reporting for as many as eight occurrences of primary melanoma. A full body and skin evaluation are the primary steps in diagnosing melanoma.
A full body-skim examination includes checking for the most common signs of melanoma formation, popularly known as the ABCDEs of melanoma. They are:
- Asymmetric shape, whereas most benign moles are symmetrical in shape,
- Borders which are uneven or irregular as compared to those of the regular moles
- Color of the mole being abnormally brown or black or blue or tan (more than one color), whereas most normal moles are either of a lighter and more uniform shade of brown or tan in color (one single color)
- Diameter of the mole being more than 6mm.
- Evolution of the mole is the most important factor to be considered when one is suspecting a possible case of melanoma. Any unusual changes that it might have undergone, pertaining to the shape, size and color, even any sensation of pain around it, should be immediately reported to the dermatologist for a check-up.
Apart from this test, another method to detect the presence of melanomas is the ‘Ugly Ducking’ test. As suggested by the name, the test is done to detect the ‘ugly duckling’ among the lesions on the body. A visual comparison is done by the specialist, comparing the diameter, thickness and color of the suspected moles with the rest of them. People with fair skin and light colored hair are tested for the ‘Little Red Riding Hood’ sign, as there may be more malignant melanomas and difficult-to-distinguish amelanotic melanomas which are unusually colored as compared to normal ones. The ones which resemble the normal moles, but are malignant, are known as ‘wolves in sheep clothing’.
Though visual diagnosis is still the most common form of diagnosis used till date, it might give rise to false positives as not all melanomas have a diameter of 6mm or more, some are smaller, and some are malignant from the very day they are apparent on the skin. To confirm the presence or absence of malignant moles, the visual detection is accompanied by examinations with dermatoscopes (Epiluminescence Microscopy) along with computerized image analysis.
Following a dermatoscopic examination, further confirmation can be done with the help of skin biopsies and if found malignant, excision is performed. Excision is followed by a thorough histologic analysis if the same. This analysis measures the thickness of the tumor and checks for the rate of cell division of the malignant cells. Breslow thickness is a measure of the tumor thickness and is used to calculate the average survival rates of patients. The relative measurements include,
- <1mm: 5-year survival is 95-100%
- 1-2mm: 5-year survival is 80-96%
- o 2.1-4mm: 5-year survival is 60-75%
- >4mm: 5-year survival is 37-50%
Another known method of determining the depth of the tumor in the body is a measurement of Clark’s level. Although, it is not as great an indicator of the outcome as the Breslow thickness, it might be used to aid the analysis. The stages as determined by Clark’s level include,
- Clark’s Level I – Confined to epidermis – also called “in situ” melanoma
- Clark’s Level II – Invasion of the papillary dermis (upper)
- Clark’s Level III – Filling of the papillary dermis (lower)
- Clark’s Level IV – Extending into the reticular dermis
- Clark’s Level V – Invasion of the subcutaneous tissue
Apart from visual and in vivo diagnostic methods, some biochemical laboratory methods are also employed to check for abnormalities and signs of malignancy in the human body. Some of them include Alanine aminotransferase (ALT) and Aspartate aminotransferase (AST) which help detecting metastasis to the bones and the liver. Similarly, the lactate dehydrogenase test also acts as a prognostic indicator towards malignancies and metastases in the lungs and liver. Chemotherapeutic treatments often cause toxic damages to the kidney and hence a creatinine level test is important to get an idea of renal health before initiating a treatment measure. For patients with severe (mostly invasive) conditions, imaging techniques like chest radiography, computed tomography (CT) scanning or magnetic resonance imaging (MRI) can be employed to detect metastases to the lungs, liver and brain.
 Staging:
Staging:

The different stages of melanomas are numbered in roman letters in order to distinguish the severity of the condition. Whether the benign tumor is confined to the tissue, or spread towards the lymph nodes or distant organs, is denoted by the TNS system. These can be summarized as follows:
- Stage 0 indicating the very initial stage of melanoma formation in situ which has not spread anywhere in the body but is confined to the epidermis, with a 5 year survival rate of more than 99%.
- Stage IA indicating a slightly invasive form of melanoma where the tumor is less than 1mm thick, without ulceration and a mitotic division of less than 1/mm2, often denoted as T1a in the TNM (Tumor, Lymph Node, Metastasis) system of classification.
- Stage IB indicating a slightly invasive form of melanoma, where the tumor is less than 1mm thick and ulcerated with primary mitotic division levels of less than or equal to 1/mm2 , also denoted as T1b. Another class of non-ulcerated tumors between 1 and 2mm thickness, are staged under T2a. It is to be noted that the 5 year survival rate for stage I of skin cancer lies between 85 and 95%.
- Stage IIA indicates a high risk melanoma with the tumor being ulcerated and lying between 1 and 2mm thickness (denoted as T2b), or non-ulcerated, measuring 2 to 4mm in thickness (denoted as T3a).
- Stage IIB indicates a high risk melanoma with the tumor being ulcerated and measuring between 2 to 4mm in thickness (denoted as T3b), or non-ulcerated with a thickness of more than 4mm (denoted as T4a). There have been no signs of spread to lymph nodes or any other organ till this stage.
- Stage IIC indicates a high risk melanoma with the tumor thickness being more than 4mm along with ulceration. There is a high possibility that the tumor may start spreading towards surrounding lymph nodes. This stage is denoted as T4b according to the TNS classification. The median 5 year survival rates for stage II of skin cancer varies between 45 to 79%.
- Stage IIIA indicates regional metastasis with the tumor being of any thickness more than 4mm, being ulcerated and has spread to one lymph node. This is denoted by N1 in the TNS system.
- Stage IIIB indicates a more severe regional metastasis with the tumor spreading to two or three lymph nodes, denoted by N2.
- Stage IIIC indicates spread of the tumor to four or more lymph nodes, denoted by N3. The median 5 year survival rate for stage III of skin cancer is low, lying between 24 to 60%.
- Stage IV indicates the most severe form of invasive cancer with distant metastasis, to the skin (M1), to the lungs and liver (M2) (M1 and M2 having normal levels of lactate dehydrogenase from lab analyses) or to distant organs (M3). This stage is the indicator for advanced malignant melanoma. The 5 year survival rates of this stage of skin cancer are the lowest, lying between 7 and 19%.
 Treatment:
Treatment:

There are several approaches to treating melanoma including surgery, immunotherapy, radiotherapy with or without chemotherapy, and adjuvant therapy. The key to employing a particular method depends on the staging of the condition along with the overall health condition of the patient. For a case of recurrent melanoma, a thorough history of the patient’s previous treatment regimens needs to be elucidated before proceeding to treatment measures.
Surgical therapy is the most common method applied to treat skin cancer, especially melanoma. For stages 0, I and IIA, surgical removal of the tumor and the affected tissues nearby, is said to be sufficient to control the growth of cells temporarily. However, stage IIA and above require additional therapy apart from just surgery, along with regular follow ups on the condition of the excised part of the skin and to stop any further chances of recurring melanoma. Generally a wide local excision (WLE) is done with 1 to 2 cm margins from the actual tumor, to keep a safe boundary during the removal of the affected tissue. This type of surgery is often specialized with very narrow margins, between .5 to 1.5mm, known as Moh’s surgery. Here, once the affected tissues are removed, they are studied by the surgeon microscopically, after being processed in a cryostat and stained with appropriate dyes. If cancerous cells are found within the borderline tissues as well, the process is repeated, till there are no more cancerous cells in the near vicinity. The rates of success with this form of surgery are very high and this surgery is recommended by most dermatologists and oncologists at the American Academy of Dermatology.
Also, involvement of lymph nodes is checked by a process known as lymphoscintigraphy, where a radioactive marker bound to a tracer molecule is injected at the site of the tumor. If lymph nodes are found to be involved, a sentinel lymph node biopsy is done to further confirm the presence of tumor cells. On getting positive results, lymph node dissection is performed, along with parallel adjuvant therapies being continued. Hence, surgery forms the main basis of treatment for all forms of melanomas. However, advanced stage metastatic malignant melanoma is the least affected by surgery and hence needs only adjuvant medical therapy along with immunotherapy in order to increase the life span of the patient.
Medications which are commonly prescribed either in combination to surgery or as follow up regimens, include, Dacarbazine (DTIC), trametinib (Mekinist), dabrafenib (Tafinlar), ipilimumab (Yervoy), vemurafenib (Zelboraf), and pembrolizumab (Keytruda), and for severe cases ( advanced malignant stages) Carboplatin and paclitaxel. Immunotherapy mainly deals with interleukins and interferons which boost the immune system and help in fighting tumor cells on their own.
In every case, an expert opinion from the oncologist and dermatologist should be taken to ensure maximum longevity and better prognosis. Supporting all these treatment regimes should be a healthy diet and a good and positive lifestyle.